
The chaos outside the medical camp. The number of patients who camp vastly exceeded my estimates, swamping the doctors and the volunteers and leading to the eventual failure of the camp.
DEV-1
Devipur Medical Camp
Devipur/Ramnagar Border Refugee Camp near Akhnoor
March 21st
| My Devipur medical camp was a
spectacular failure, but paradoxically set the stage for the success of
the following 5 camps. Devipur is a refugee camp situated about 15
kms from the border with Pakistan. These were refugees who had fled
their homes and farms along the Pakistan border after the Kargil War in
1999. Since that war, India and Pakistan had conducted a
never-ending tit-for-tat warfare in which they fired shells at each
other's positions. Occasionally, they hit bunkers, but usually, they
hit empty fields and sometime villages. Indeed, homes and schools in
these villages still bear bullet holes and shell damage from these
cross-border fire fights. In 2002, the 2-countries agree to a
cease-fire. However, the villagers did not return to their homes,
partly because they feared a re-surgence in violence, but mostly because
they did not have the money to re-seed and re-till their abandoned
farmlands. Essentially, they have been waiting for government
funding to re-settle into their villages, although some started to return
to their villages when I left Jammu in July 2004. |
|
|
The chaos outside the medical camp. The number of patients who camp vastly exceeded my estimates, swamping the doctors and the volunteers and leading to the eventual failure of the camp. |
|
DEV-1 |
| At the time of the camp in March, it was inhabited by about 5,000 village refugees, plus about 4,000 in the neighboring Ramnagar camp. We publicized heavily, and suffered because of it. I expected about 200 patients, but we were swamped by well over 500 patients. I had 8 doctors, but there were problems with their schedules and transportation. I did not have trained people who could fill prescriptions in an efficient manner. And worst of all, the local volunteers I recruited to manage the patient flow started letting their friends and family "cut in line," which caused a great deal of havoc and even loud arguments between the volunteers and the patients. I was not happy, but there was nothing we could do but slog through. I estimate that only 100 out of 500 patients received medicines that significantly helped them. The rest only received prescriptions, or symptomatic treatments such as PCM, Nimesulide, Rofecoxib, Diclofenac, etc. The camp was a personal embarrassment for me. At later camps, I drilled the volunteers to make sure they handled the patient flow efficiently, and I set up our mini-pharmacy so that the prescriptions could be filled as fast as the combined doctors were writing them. |
 |
|
Some of the tents of the Devipur Border Migrant (Refugee) camp. There are about 800 families (5,000 occupants) living in 900 tents in Devipur. Ramnagar, off frame to the left, has about 600 families (4,000 occuptants) in 800 tents. |
|
DEV-2 |
 |
|
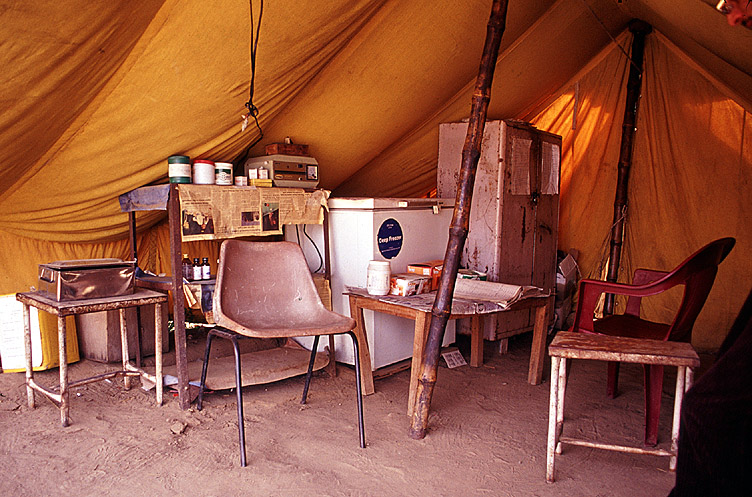
The sorry state of the Rural Health Services. An MBBS doctor, Dr. Jadish Lal, is supposed to attend this camp 2 days a week, but residents of the border refugee camp say he rarely comes. I later learned that Dr. Lal has a private clinic in Akhnoor town. He see poor patients during the day while serving the government, and compels them to see him in the evening at his clinic, so that he can make money from them. He then writes prescriptions for brand-name medicines that are sold within his clinic. So, he butters all 3 sides of the toast: 1) he draws a government salary, 2) he makes money from patients being referred to his private clinic, 3) he profits by selling his own prescriptions at the MRP (maximum retail price). |
|
DEV-3 |
 |
|
An example of Indian bureacracy: the deputation order for the gynaecologists from the Government Medical College Principal (i.e. Dean). |
|
DEV-4 |
 |
|
Dr. Deepak Pandita, opthamologist, sees a patient. |
|
DEV-5 |
 |
|
Dr. Mandeep Singh, dental surgeon, gives consultation. |
|
DEV-6 |
 |
|
My friends from KGNT do publicity a few days before the camp. |
|
DEV-6 |